
24 results
The kynurenine pathway in schizophrenia, bipolar disorder, and major depressive disorder: a systematic review and meta-analysis of cerebrospinal fluid studies
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S620
-
- Article
-
- You have access
- Open access
- Export citation
Precision in bipolar disorders
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S5
-
- Article
-
- You have access
- Open access
- Export citation
Does bipolar disorder differ from other mental illnesses in terms of emotion dysregulation? A systematic review and meta-analysis
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S571-S572
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Emotion regulation (ER) is the ability to assess, monitor, or modify emotional reactions to achieve a goal (Gross. Psychological inquiry 2015; 26 1-26). When ER strategies are rigidly or maladaptively applied, emotional dysregulation (ED) can occur (Thompson. Development and psychopathology 2019; 31 805-815). ED is common in people diagnosed with bipolar disorder (BD), but it can also be described in other clinical populations given its transdiagnostic nature. Numerous aspects of ED have been described in BD (De Prisco et al. Neuroscience & Biobehavioral Reviews 2022; 104914), but it is unclear whether these manifest similarly in other conditions such as major depressive disorder (MDD) or borderline personality disorder (BPD), or whether they are specific to BD.
ObjectivesThe objective of this systematic review and meta-analysis is to examine the literature comparing BD with other psychiatric disorders in terms of ED, focusing on those studies using validated clinical tools.
MethodsA systematic search from inception to April 28th, 2022, was conducted exploring the PubMed/MEDLINE,EMBASE, Scopus, and PsycINFO databases. Those studies providing quantitative data on ED in people diagnosed with BD and compared with clinical groups were eligible for inclusion. No restriction about age, sample size, or language were applied. Random effect meta-analyses were conducted, and effect sizes were calculated as standardized mean differences (SMD).
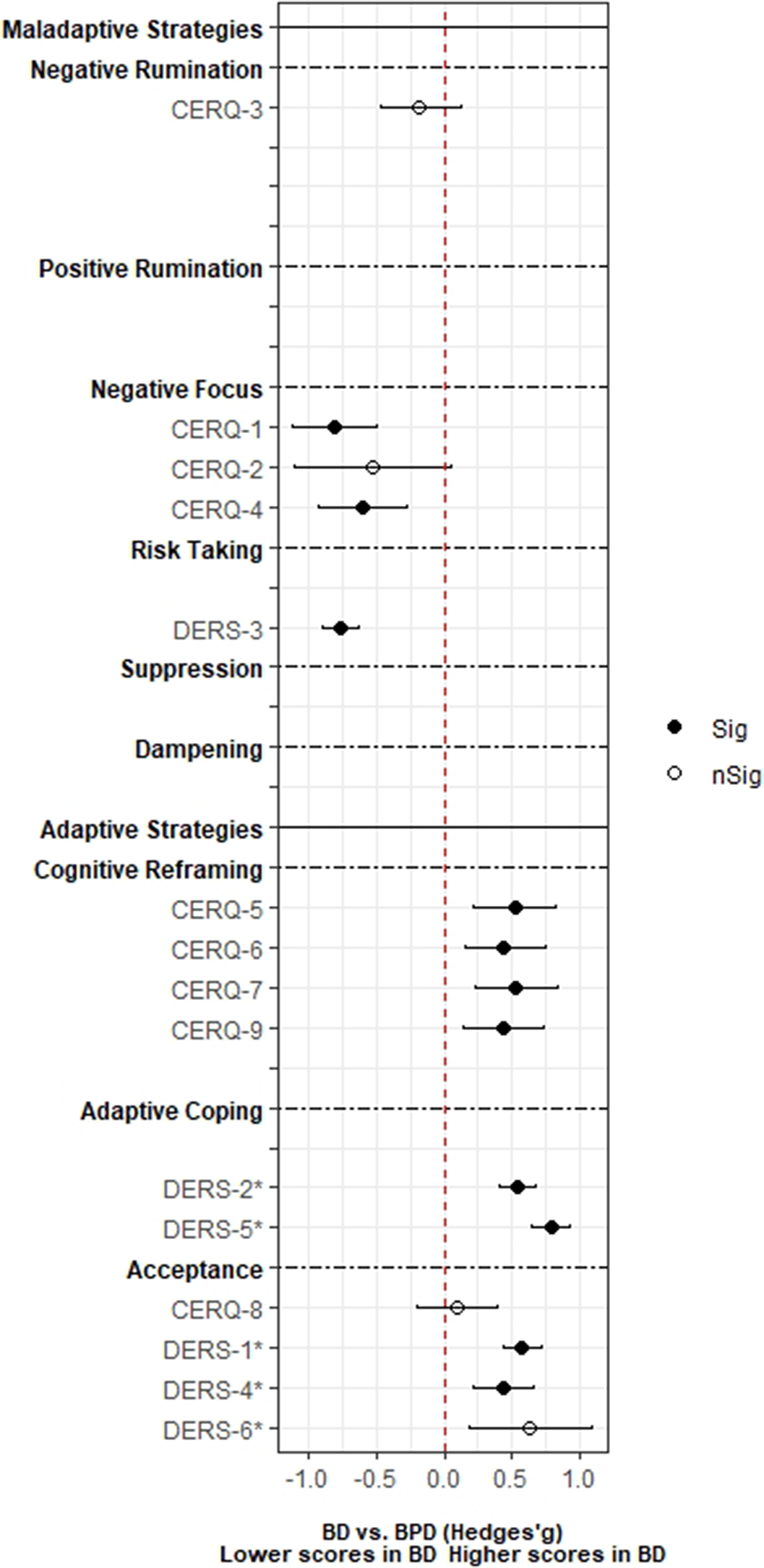
ResultsA total of 3,239 records was identified and, after duplicate removal and title/abstract evaluation, 112 were explored at the full text. Twenty-nine studies were finally included, and it was possible to perform a meta-analysis with twenty-two (145 comparisons) of them. Only studies comparing BD with MDD, and BPD provided sufficient data to perform a meta-analysis. People with BD did not differ from people with MDD in most of the comparisons considered. However, BD patients presented higher positive rumination (two comparisons: SMD=0.46; CI=0.27, 0.64; p=8.5e-07; I2=0%; and SMD=0.34; CI=0.15, 0.52; p=2.7e-04; I2=0%) and risk-taking behaviors (SMD=0.48; CI=0.27, 0.69; p=8.11e-06; I2=0%). In contrast, people with BPD displayed an overall higher degree of ED (SMD=-1.22; CI=-1.94, -0.5; p=9.1e-04; I2= 90.7) and used fewer adaptive ER strategies. Additionally, higher levels of self-blaming (SMD=-0.80; CI=-1.11, -0.50; p=2.68e-07; I2=0) and impulsive behavior (SMD=-0.76; CI=-0.89, -0.63; p=5.4e-29; I2=0) were observed.
Image:
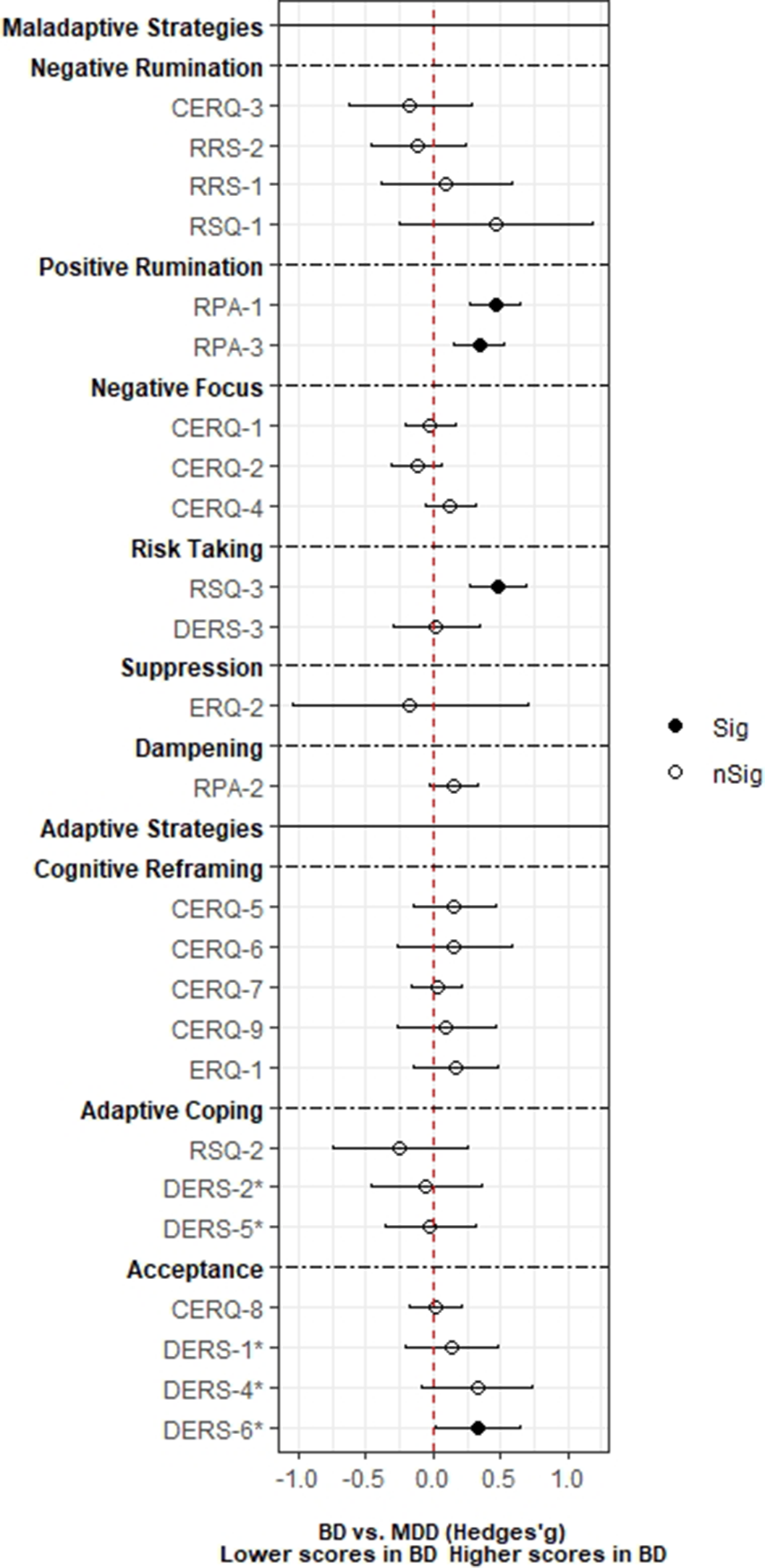
Image 2:
 Conclusions
ConclusionsED is a trans-diagnostic construct that spans a continuum of different psychiatric disorders. Outlining the specific clinical features of one disorder versus another may help future research to increase our knowledge of these issues and develop new treatment strategies to reduce the clinical burden of these patients.
Disclosure of InterestM. De Prisco: None Declared, V. Oliva: None Declared, G. Fico Grant / Research support from: “La Caixa” Foundation (ID 100010434 - fellowship code LCF/BQ/DR21/11880019), Consultant of: Angelini, Janssen-Cilag and Lundbeck, J. Radua Grant / Research support from: Spanish Ministry of Science and Innovation (PI19/00394, CPII19/00009) integrated into the Plan Nacional de I+D+I and co-financed by the ISCIII-Subdirección General de Evaluación and the Fondo Europeo de Desarrollo Regional (FEDER) and the Instituto de Salud Carlos III, I. Grande Grant / Research support from: Spanish Ministry of Science and Innovation (MCIN) (PI19/00954) integrated into the Plan Nacional de I+D+I and cofinanced by the ISCIII-Subdirección General de Evaluación y el Fondos Europeos de la Unión Europea (FEDER, FSE, Next Generation EU/Plan de Recuperación Transformación y Resiliencia_PRTR ); the Instituto de Salud Carlos III; the CIBER of Mental Health (CIBERSAM); and the the Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement (2017 SGR 1365), CERCA Programme / Generalitat de Catalunya as well as the Fundació Clínic per la Recerca Biomèdica (Pons Bartran 2022-FRCB_PB1_2022), Consultant of: ADAMED, Angelini, Casen Recordati, Ferrer, Janssen Cilag, and Lundbeck, Lundbeck-Otsuka, Luye, SEI Healthcare, N. Roberto: None Declared, G. Anmella Grant / Research support from: Rio Hortega 2021 grant (CM21/00017) from the Spanish Ministry of Health financed by the Instituto de Salud Carlos III (ISCIII) and co-financed by the Fondo Social Europeo Plus (FSE+), Consultant of: Janssen-Cilag, Lundbeck, Lundbeck/Otsuka, and Angelini, D. Hidalgo-Mazzei Grant / Research support from: Juan Rodés JR18/00021 granted by the Instituto de Salud Carlos III (ISCIII), M. Fornaro: None Declared, A. de Bartolomeis Consultant of: Janssen, Lundbeck, and Otsuka and lecture fees for educational meeting from Chiesi, Lundbeck, Roche, Sunovion, Vitria, Recordati, Angelini and Takeda; he has served on advisory boards for Eli Lilly, Jansen, Lundbeck, Otsuka, Roche, and Takeda, Chiesi, Recordati, Angelini, Vitria, A. Serretti Consultant of: Abbott, Abbvie, Angelini, AstraZeneca, Clinical Data, Boehringer, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Innovapharma, Italfarmaco, Janssen, Lundbeck, Naurex, Pfizer, Polifarma, Sanofi, Servier, and Taliaz, E. Vieta Grant / Research support from: Spanish Ministry of Science and Innovation (PI18/00805, PI21/00787) integrated into the Plan Nacional de I+D+I and co-financed by the ISCIII-Subdirección General de Evaluación and the Fondo Europeo de Desarrollo Regional (FEDER); the Instituto de Salud Carlos III; the CIBER of Mental Health (CIBERSAM); the Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement (2017 SGR 1365), the CERCA Programme, and the Departament de Salut de la Generalitat de Catalunya for the PERIS grant SLT006/17/00357. Thanks the support of the European Union Horizon 2020 research and innovation program (EU.3.1.1. Understanding health, wellbeing and disease: Grant No 754907 and EU.3.1.3. Treating and managing disease: Grant No 945151), Consultant of: AB-Biotics, AbbVie, Angelini, Biogen, Boehringer-Ingelheim, Celon Pharma, Dainippon Sumitomo Pharma, Ethypharm, Ferrer, Gedeon Richter, GH Research, Glaxo-Smith Kline, Janssen, Lundbeck, Medincell, Novartis, Orion Corporation, Organon, Otsuka, Rovi, Sage, Sanofi-Aventis, Sunovion, Takeda, and Viatris, A. Murru Grant / Research support from: Spanish Ministry of Science and Innovation (PI19/00672) integrated into the Plan Nacional de I+D+I and co-financed by the ISCIII-Subdirección General de Evaluación and the Fondo Europeo de Desarrollo Regional (FEDER), Consultant of: Angelini, Idorsia, Lundbeck, Pfizer, Takeda


Vickybot, a chatbot for anxiety-depressive symptoms and work-related burnout
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S109-S110
-
- Article
-
- You have access
- Open access
- Export citation
Psychiatric comorbidity profiles among suicidal attempters: A cohort study
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S318-S319
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
More than 700,000 people die by suicide in 2019 globally (World Health Organitation 2021). Mental health problems constitute a risk factor for suicidal behavior and death by suicide (Hoertel et al. Mol Psychiatry 2015; 20 718–726). Different mental disorders have been related to different forms of suicidal ideation and behavior (Conejero et al. Curr Psychiatry Rep 2018; 20, 33) (Quevedo et al. Compr Psychiatry 2020; 102 152194). However, little is known on comorbidity profiles among suicide attempters.
ObjectivesThe aim of our work was to identify the psychiatric comorbidity profiles of individuals who were admitted a hospital emergency department due to a suicide attempt. Moreover, it intended to know their clinical characteristics according to comorbidity profile.
MethodsA sample of 683 attempters (71.30% female; M age= 40.85, SD= 15.48) from the SURVIVE study was used. Patients were assessed within the 15 days after emergency department admission. Sociodemographic (i.e., sex, age, marital status and employment status) and clinical data were collected. The International Neuropsychiatric Interview (MINI) was used to assess DSM-V Axis 1 mental health diagnoses and the Columbia Suicide Rating Scale (C-SSRS) to assess suicidal ideation and behavior. The Acquired Capacity for Suicide-Fear of Death Scale (ACSS-FAD), the Patient Health Questionnaire (PHQ-9) to assess the frequency of depressive symptoms during the past 2 weeks, and the General Anxiety Disorder-7 (GAD-7) scale to assess symptoms of worry and anxiety were also conducted. For the identification of comorbidity profiles, latent class analysis framework was followed considering diagnosis to each individual disorder as clustering variables. On the other hand, binary logistic regression was used to study the relationship between comorbidity profile membership and clinical factors.
ResultsTwo classes were found (Class I= mild symptomatology class, mainly featured by emotional disorder endorsement; and Class II= high comorbidity class, featured by a wide amount of endorsed diagnoses) (see figure 1). Individuals from the High comorbidity class were more likely to be female (OR= 0.98, p<.05), younger in age (OR= 0.52, p< .01), with more depressive symptoms (OR=1.09, p<.001) and have greater impulsivity (OR= 1.01, p<.05).
Image:
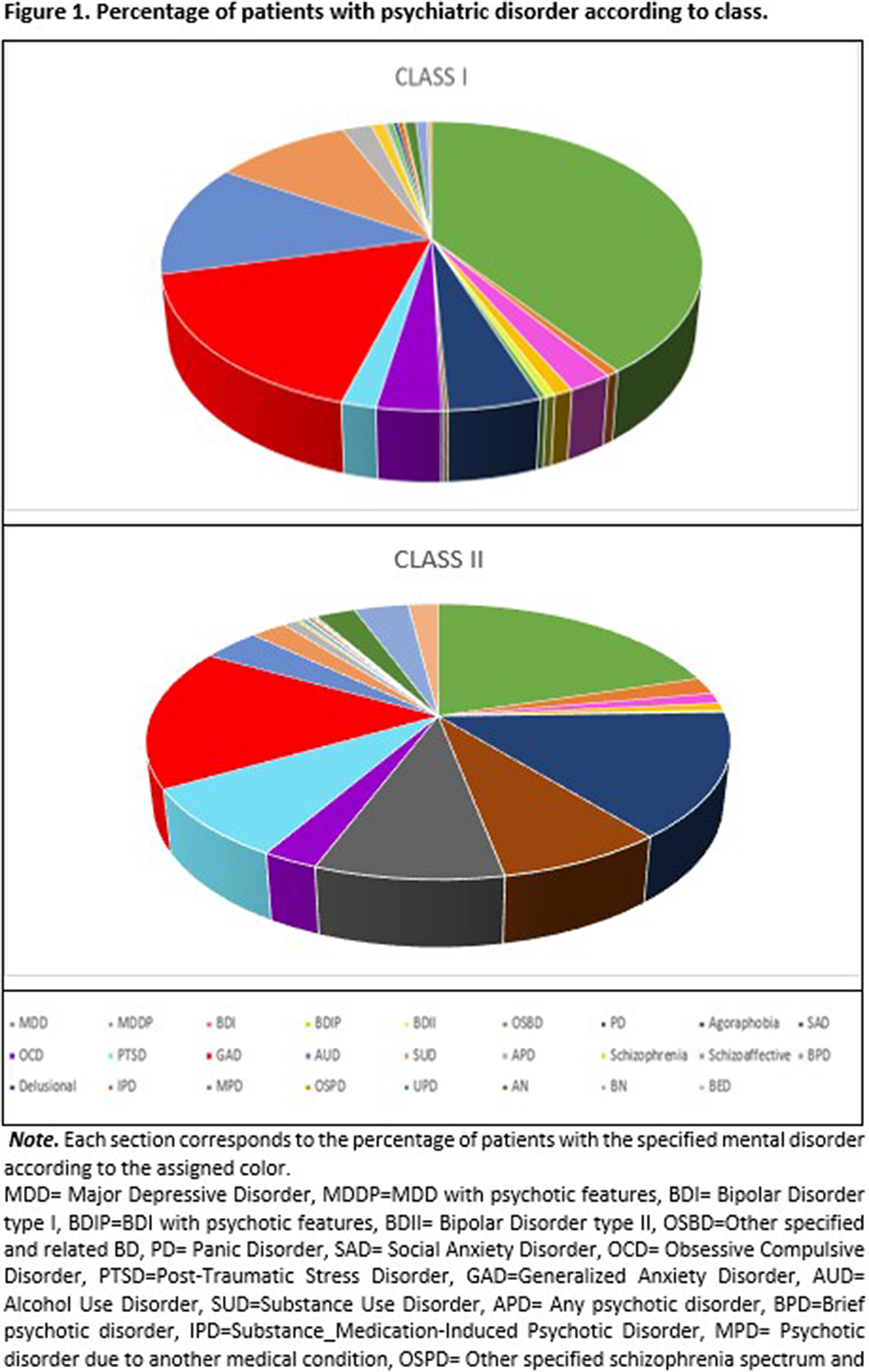 Conclusions
ConclusionsWe found two profiles of people with suicidal behavior based on the presence of mental disorders. Each of the suicidal subtypes had different associated risk factors. They also had a different profile of suicidal behavior.
Disclosure of InterestNone Declared

Parkinson’s Disease and Bipolar Disorder: a case report and narrative review
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S480
-
- Article
-
- You have access
- Open access
- Export citation
P03-321 Antipsychotic Polipharmacy in Schizophrenic Inpatients
-
- Journal:
- European Psychiatry / Volume 25 / Issue S1 / 2010
- Published online by Cambridge University Press:
- 17 April 2020, 25-E927
-
- Article
-
- You have access
- Export citation
P03-333 - Electrocardiographic Alterations in Patients in Treatment with Clozapine
-
- Journal:
- European Psychiatry / Volume 25 / Issue S1 / 2010
- Published online by Cambridge University Press:
- 17 April 2020, 25-E939
-
- Article
-
- You have access
- Export citation
The burden of mental disorders in primary care
-
- Journal:
- European Psychiatry / Volume 26 / Issue 7 / October 2011
- Published online by Cambridge University Press:
- 16 April 2020, pp. 428-435
-
- Article
- Export citation
Remission and functioning after two years undergoing Long-Acting Injectable Risperidone (LAIR) in recent-onset schizophrenia
-
- Journal:
- European Psychiatry / Volume 26 / Issue S2 / March 2011
- Published online by Cambridge University Press:
- 16 April 2020, p. 1344
-
- Article
-
- You have access
- Export citation
is the Brief Psychotic Disorder a Distinct Nosologic Entity?: A Longitudinal Study of 80 Patients
-
- Journal:
- European Psychiatry / Volume 24 / Issue S1 / January 2009
- Published online by Cambridge University Press:
- 16 April 2020, 24-E1188
-
- Article
-
- You have access
- Export citation
The Real World Costs of Asenapine in Manic Episodes in the Manacor Study
-
- Journal:
- European Psychiatry / Volume 30 / Issue S1 / March 2015
- Published online by Cambridge University Press:
- 15 April 2020, p. 1
-
- Article
-
- You have access
- Export citation
Asenapine prescribing patterns in the treatment of manic in- and outpatients: Results from the MANACOR study
-
- Journal:
- European Psychiatry / Volume 30 / Issue 4 / June 2015
- Published online by Cambridge University Press:
- 15 April 2020, pp. 528-534
-
- Article
- Export citation
P-179 - Brain-derived Neurotrophic Factor as a Biomarker of Clinical Response in Bipolar Disorder: 16 Week Follow-up Study
-
- Journal:
- European Psychiatry / Volume 27 / Issue S1 / 2012
- Published online by Cambridge University Press:
- 15 April 2020, p. 1
-
- Article
-
- You have access
- Export citation
1588 – Interleukin-6 As a Biomarker Of The Model Of Staging In Bipolar Disorder
-
- Journal:
- European Psychiatry / Volume 28 / Issue S1 / 2013
- Published online by Cambridge University Press:
- 15 April 2020, 28-E874
-
- Article
-
- You have access
- Export citation
High Cognitive Reserve in Bipolar Disorders as a Moderator of Neurocognitive Impairment
-
- Journal:
- European Psychiatry / Volume 41 / Issue S1 / April 2017
- Published online by Cambridge University Press:
- 23 March 2020, p. S116
-
- Article
-
- You have access
- Export citation
Staging in Bipolar Disorder: Clinical, Biochemical, and Functional Correlates
-
- Journal:
- European Psychiatry / Volume 41 / Issue S1 / April 2017
- Published online by Cambridge University Press:
- 23 March 2020, p. S34
-
- Article
-
- You have access
- Export citation
Use of benzodiazepines and cognitive performance in primary care patients with first cognitive complaints
-
- Journal:
- International Psychogeriatrics / Volume 30 / Issue 4 / April 2018
- Published online by Cambridge University Press:
- 10 November 2017, pp. 597-601
-
- Article
- Export citation
The Clinical Implications Of Cognitive Impairment and Allostatic Load in Bipolar Disorder
-
- Journal:
- European Psychiatry / Volume 28 / Issue 1 / January 2013
- Published online by Cambridge University Press:
- 24 April 2012, pp. 21-29
-
- Article
- Export citation
High power laser development and experimental applications to X-ray lasers, and short pulse energy transport
-
- Journal:
- Laser and Particle Beams / Volume 8 / Issue 1-2 / January 1990
- Published online by Cambridge University Press:
- 09 March 2009, pp. 19-25
-
- Article
- Export citation
